Do migrants always live longer than natives? Finnish migrants in Sweden
Abstract
Migrants’ health depends on factors both at their places of origin and destination. Finnish migrant men living in Sweden have total mortality rates falling between those of the Finnish and Swedish populations. Migrant women, however, have slightly higher total mortality than both populations. However, their alcohol- and smoking-related mortality levels lie between those of Swedes and Finns. Overall, migrants’ health behaviours are influenced, positively or negatively, by social conditions at both origin and destination.
Article
Department of Public Health Sciences, Stockholm University; Aging Research Center (ARC), Karolinska Institutet
Population Research Unit, University of Helsinki
Department of Public Health Sciences, Stockholm University
Population Research Unit, University of Helsinki; The Max Planck Institute for Demographic Research
Migrants’ health depends on factors both at their places of origin and destination. Finnish migrant men living in Sweden have total mortality rates falling between those of the Finnish and Swedish populations. Migrant women, however, have slightly higher total mortality than both populations. However, their alcohol- and smoking-related mortality levels lie between those of Swedes and Finns. Overall, migrants’ health behaviours are influenced, positively or negatively, by social conditions at both origin and destination.
migration, migrant, health, alcohol, smoking, mortality, Sweden, Finland
Table of contents
- Appendix A References
1.
In France, immigrants have a lower mortality risk than the native-born population—a seemingly surprising outcome given that they generally come from more socio-economically disadvantaged backgrounds. One reason for this is that migrants are among the healthier individuals in their countries of origin. Do we observe the same paradox when immigrants and natives are born in similar countries? This is the question Olof Östergren and his colleagues ask as they examine the mortality risk of Finnish immigrants in Sweden.
Migrants comprise a growing part of populations in many high-income countries, which has sparked increasing interest in understanding the determinants of their health. Researchers tend to agree that migrant health is shaped by factors in the country of origin, the migration event, circumstances surrounding migration, and factors in the country of destination. It is therefore important to consider not only the specific historical and contextual factors surrounding the migration event but also migrant health in relation to both origin and destination populations. Here, we examine the mortality of Finnish migrants in Sweden, whose life expectancy is several years shorter than that of the native population of Sweden.1
1.1. Finnish migration to Sweden: a long story short
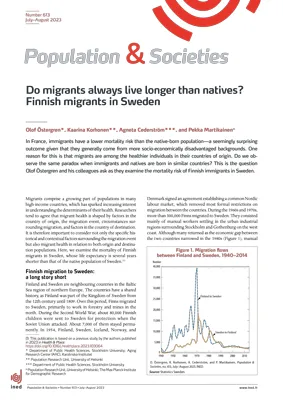
Finland and Sweden are neighbouring countries in the Baltic Sea region of northern Europe. The countries have a shared history, as Finland was part of the Kingdom of Sweden from the 12th century until 1809. Over this period, Finns migrated to Sweden, primarily to work in forestry and mines in the north. During the Second World War, about 80,000 Finnish children were sent to Sweden for protection when the Soviet Union attacked. About 7,000 of them stayed permanently. In 1954, Finland, Sweden, Iceland, Norway, and Denmark signed an agreement establishing a common Nordic labour market, which removed most formal restrictions on migration between the countries. During the 1960s and 1970s, more than 300,000 Finns migrated to Sweden. They consisted mainly of manual workers settling in the urban industrial regions surrounding Stockholm and Gothenburg on the west coast. Although many returned as the economic gap between the two countries narrowed in the 1980s (Figure 1), manual workers are still predominant among first-generation Finnish migrants in Sweden. Finns remained the largest first-generation migrant group in Sweden until 2017; and in 2022, 133,083 Finnish-born persons were living in Sweden, about 6.2% of the foreign-born population.

1.2. Health differences between Finnish migrants and native Swedes
International migrants tend to have lower mortality rates than resident populations, a phenomenon sometimes referred to as the migrant mortality advantage [1]. However, this is not always the case. For example, Finnish migrants in Sweden, particularly men, have higher mortality rates than the native population. What might account for these mortality differentials between migrants and natives? Here, we explore several explanations related to the specific characteristics of Finnish migration to Sweden.
First, thehealthy migrant effect suggests that migration is challenging, requiring varying degrees of resources and physical and mental fortitude. Consequently, only comparatively healthy individuals migrate, which contributes to better health and lower mortality among migrants in the destination country [2]. The healthy migrant effect is probably stronger when the barriers to migration are more pronounced. Given the fewer obstacles to migration between the Nordic countries, this effect is unlikely to play a dominant role in mortality rates among Finnish migrants in Sweden.
The salmon bias effect is a second possible explanation for the migrant mortality advantage. If migrants in poor health return to their country of origin before dying, their death will not be counted in the country of destination. If this is common, the number of deaths among migrants can appear lower than among natives—not because migrants live longer, but because these deaths occur where they cannot be observed. A large number of Finnish migrants returned to Finland in the 1980s (Figure 1). If the group that returned had worse health than the group that stayed in Sweden, this return migration may have led to lower mortality rates among those that remained.
A third explanation pertains to cultural effects, which suggests that norms and behaviours established before migration and maintained afterwards contribute to health differences between migrants and natives [3]. Additionally, these differences between migrants and the majority population at the destination may diminish over time as both groups interact [4], which can be either beneficial or detrimental to migrant health.
This third explanation seems particularly relevant for our setting. Harmful behaviours, such as smoking and drinking, are more prevalent in Finland than in Sweden. A recent study found that about 1.5 of the 2-year difference in life expectancy (at ages 25–79) between Finland and Sweden can be attributed to alcohol- and smoking-related mortality among men, though only modest differences (0.1 years) in overall life expectancy at the same ages were observed for women [5]. The Finnish migrants under consideration here, who typically arrived in Sweden at working age, might maintain habits established before migration, leading to higher mortality.
Finally, reflecting the dominance of manual workers during the peak of Finnish migration to Sweden, Finnish migrants in Sweden occupy on average lower socio-economic positions than those of both the Swedish and Finnish native populations: they are less educated, have lower income, and are more often unmarried (Figure 2). Because socio-economic position and marital status have strong associations with mortality and health behaviours, we would expect higher mortality among Finnish migrants. To evaluate the possible causes of mortality variations among Finnish migrants, we use rich administrative register data in both Finland and Sweden (Box 1).

1.3. Finding matched controls in two countries
Using the total population register in Sweden, we identified all Finnish-born individuals residing in Sweden in 1999, aged 40–64, when they were likely to be active in the labour market. They largely consisted of working-class individuals who arrived as adults or young adults. The median age at arrival was 21 years, and 72% were 18 or older at migration.
Figure 2 shows that Finnish migrants are more often unmarried, have less education, and occupy the lowest income quintiles than native Finnish and native Swedish in the full population. Marital status, education, and income are associated with mortality. To calculate differences by migrant status, we need to compare migrants with natives having similar characteristics. For each Finnish migrant, we draw five random controls in Finland and five in Sweden in the register who share the exact combination of sex, age, marital status, education, and income (presented as the matched samples2 in Figure 2). This procedure allows us to compare migrants’ mortality risks with two reference populations—those at origin and destination—net of any differences in sociodemographic conditions between the populations.
1.4. Mortality patterns of Finnish migrants lie between those at origin and destination
Figure 3 illustrates male and female mortality rates between 2000 and 2017 of migrants, native Finns, and native Swedes, observing all-cause mortality as well as mortality from smoking-3 and alcohol-related4 causes of death. The causes were selected based on evidence that smoking and alcohol consumption contribute to differences in life expectancy between the national populations of Finland and Sweden [5]. Mortality rates are higher among men than among women.5 The solid bars present the observed mortality levels of the three populations, while the diamonds present mortality levels of the native Swedes and Finns, who have similar characteristics as the migrants (matched reference samples). The mortality levels of the matched reference samples are higher than in the observed total population, indicating that part of the mortality disadvantage of migrants is attributable to less favourable sociodemographic characteristics. Finnish migrants in Sweden have mortality patterns that lie between the origin and the destination. The all-cause mortality rate in the matched sample is 172.3 for native Finns, 149.9 for the migrants, and 116.0 for native Swedes. We found a similar gradient for smoking- and alcohol-related mortality. For Finnish men, adjustment of their drinking and smoking habits to resemble those of the Swedish population may have contributed to lower overall mortality. Selective return migration might also contribute to the pattern: migrants who experienced more difficulty adapting may also have been more likely to return to Finland. The group remaining in Sweden may therefore be likely to smoke and drink less, and therefore be in better health.

Unlike the mortality differences between men, those between the groups of women are generally small. Migrant women have somewhat higher all-cause mortality than that of both Swedes and Finns, although the differences have largely to do with sociodemographic conditions. Like the pattern observed for men, migrant women have alcohol- and smoking-related mortality rates in between those of the populations of Finland and Sweden. Among both men and women, alcohol-related mortality is higher in Finland than in Sweden. The female mortality rate from alcohol-related causes in the matched sample is 6.0 (per 10,000 person-years) in Finland, 4.2 among migrants, and 2.2 in Sweden. On the other hand, Swedish women have a higher smoking-related mortality rate than Finnish women. The mortality rate from smoking-related causes in the matched sample is 6.7 in Finland, 9.4 among migrants, and 10.2 in Sweden. A mortality rate that lies between the two countries in this case implies that the migrant women have a higher mortality rate from smoking-related causes than their Finnish counterparts. Migration to Sweden thus seems to be associated with lower alcohol-related mortality in later life but higher smoking-related mortality among women.
Like male migrants’ patterns, those among migrant women indicate that their habits align more closely to those of Swedish women compared with their Finnish counterparts who did not migrate. However, unlike among men, this alignment has not affected overall mortality but rather has changed the composition of the causes of death. The processes of behavioural convergence and selective return migration can be similar among men and women but have different impacts on health.
1.5. The migrant mortality advantage is not universal
Overall, our findings point to the importance of considering the specific context of migration when drawing conclusions about the determinants of migrant health. In many contexts, the healthy migrant effect is relevant, but given the context of Finnish migration to Sweden, it is probably less important than cultural factors, such as health behaviours. Our results are consistent with the notion that behavioural adaptation may be key for migrant health, although we cannot rule out the possibility that migrants who have difficulty settling in Sweden may also be more likely to retain their health behaviours and return to Finland. Such selective return migration may be a central factor in contexts of free mobility, such as the Nordic countries but also the Schengen Area.
Migrants’ mobility between contexts presents challenges when studying them based on data sources from a single context. By broadening and comparing those sources and contexts, we discover that migrant’s behavioural patterns exhibit similarities to those in both the origin and destination populations. Depending on the specific conditions at origin and destination, adapting to local behaviours can be beneficial or detrimental for migrant health.
1.5.1. Box 1. Administrative register data in Finland and Sweden
Extensive population registers are a prominent feature of the Nordic administrative model. Government bodies routinely collect data on demographic processes, living conditions, economic activity, healthcare use, etc. Although these data are typically maintained by different agencies, it is possible to link the data at the individual level using the unique personal identity number assigned at birth or upon immigration, introduced in Sweden in 1947 and in Finland during the 1960s. Anonymized register data can be used for research after a lengthy process of ethical and legal vetting, where the scientific merits of the research are evaluated. For a discussion on the use of register data in Nordic comparative research on health inequalities, see Van Der Wel et al. [6]. Here, we use individual data on sex, age, marital status, education, and disposable household income, obtained by linking several administrative registers.
Appendix A References
- [1] Aldridge R. W., Nellums L. B., Bartlett S., Barr A. L., Patel P., Burns R. et al., 2018,
- Global patterns of mortality in international migrants: A systematic review and meta-analysis, The Lancet, 392(10164), 2553–2566. https://doi.org/10.1016/S0140-6736(18)32781-8
- [2] Wallace M., Wilson B., 2019, Migrant mortality advantage versus origin and the selection hypothesis, Population and Development Review, 45(4), 767–794. https://doi.org/10.1111/padr.12298
- [3] Guillot M., Khlat M., Elo I., Solignac M., Wallace M., 2018, Understanding age variations in the migrant mortality advantage: An international comparative perspective, PLOS One, 13(6), e0199669. https://doi.org/10.1371/journal.pone.0199669
- [4] Antecol H., Bedard K., 2006, Unhealthy assimilation: Why do immigrants converge to American health status levels?Demography, 43(2), 337–360. https://doi.org/10.1353/dem.2006.0011
- [5] Östergren O., Martikainen P., Tarkiainen L., Elstad J. I., Brønnum-Hansen H., 2019, Contribution of smoking and alcohol consumption to income differences in life expectancy: Evidence using Danish, Finnish, Norwegian and Swedish register data, Journal of Epidemiology and Community Health, jech-2018-211640. http://dx.doi.org/10.1136/jech-2018-211640
- [6] Van Der Wel K. A., Östergren O., Lundberg O., Korhonen K., Martikainen P., Andersen A. M. N. et al., 2019, A gold mine, but still no Klondike: Nordic register data in health inequalities research, Scandinavian Journal of Public Health, 1–13. http://dx.doi.org/10.1177/1403494819858046
This publication is based on a previous study by the authors published in 2023 in Health & Place: https://doi.org/10.1016/j.healthplace.2023.103064
See the Online Appendix for an extensive account of the matching procedure. https://doi.org/10.34847/nkl.5f547498
Smoking-related deaths were identified by malignant neoplasms of respiratory and intrathoracic organs (ICD-10 codes C30–C39) or chronic lower respiratory diseases (J40–J47) as underlying causes of death.
Alcohol-related deaths were identified by deaths from the following underlying or contributing causes: alcohol-related disorders (ICD-10, F10.09), degeneration of nervous system due to alcohol (G31.2), alcoholic cardiomyopathy (I42.6), alcoholic gastritis (K29.2), alcoholic liver disease (K70), alcohol-induced acute pancreatitis (K85.2), and alcohol-induced chronic pancreatitis (K86.0).
The matched samples are not comparable by gender. The matching process sets the distribution of socio-economic conditions in all groups to the observed distribution among Finnish migrants. Because male migrants occupy more disadvantaged positions than female migrants (Figure 2), the matched samples overestimate the gender difference in mortality in the matched non-migrant groups.
Author(s)
Olof Östergren (Department of Public Health Sciences, Stockholm University; Aging Research Center (ARC), Karolinska Institutet)
Kaarina Korhonen (Population Research Unit, University of Helsinki)
Agneta Cederström (Department of Public Health Sciences, Stockholm University)
Pekka Martikainen (Population Research Unit, University of Helsinki; The Max Planck Institute for Demographic Research)